

Assessment of various lumbosacral spine abnormalities on magnetic resonance imaging scans of patients with low back pain
Article Sidebar
Abstract Views | PDF/EPUB Downloads: 1133 / 231 / 685
Main Article Content
Abstract
Background: Low back pain (LBP) is a cardinal sign of many lumbosacral spine abnormalities. Magnetic resonance imaging (MRI) has revolutionised the management of LBP through precise diagnosis and accurate definition of the extent of the problem.
Aim: This study was carried out to determine the lumbosacral spine abnormalities on MRI scans of patients with LBP.
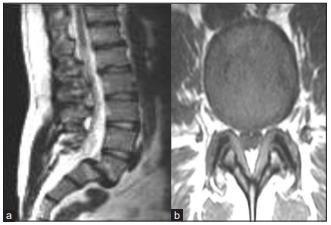
Methods: The prospective study was conducted within 4 years at the MRI suite of the Department of Radiology, Ahmadu Bello University Teaching Hospital, Zaria. This study included 200 patients who had LBP on whom MRI scan was performed. All MRI scans were done with permanent magnet 0.2 T ‘open’ MRI unit. The images were stored in a computer and subsequently viewed on the screen.
Results: The MRI findings of 200 patients involved in the study showed that more males (124 [62%]) were affected than females (76 [38%]). The age of the patients ranged from 11 to 80 years, with a mean of 47.8 (standard deviation 1.4). The peak incidence of LBP was (55 [27.5%]) in the fourth and fifth decade of life. Majority of the patients (172 [86%]) had intervertebral disc prolapse/herniation. Thecal sac, spinal cord (at L1/L2 only) and cauda equina were compressed in 159 (92.4%), 4 (2.3%) and 73 (42.3%) patients, respectively. Compression of multiple structures in the spinal canal was seen in 64 (37%) patients.
Conclusion: MRI examination has improved the management of patients with LBP, and the results obtained from this study will assist clinicians to quantitatively evaluate patients with LBP.
Downloads
Article Details
The journal grants the right to make small numbers of printed copies for their personal non-commercial use under Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported License.
References
1. Galukande M, Muwazi S, Mugisa DB. Aetiology of low back pain in Mulago Hospital, Uganda. Afr Health Sci 2005;5:164‑7.
2. Michael NB, Steven C. Low back pain. Radiology 2000;217:321‑30.
3. Weber AL. History of head and neck radiology: Past, present, and future. Radiology 2001;218:15‑24.
4. Edmond SL, Felson DT. Prevalence of back symptoms in elders. J Rheumatol 2000;27:220‑5.
5. Sikiru L, Shmaila H. Prevalence and risk factors of low back pain among nurses in Africa: Nigerian and Ethiopian specialized hospitals survey study. East Afr J Public Health 2009;1:6.
6. Jarvik JG, Deyo RA. Diagnostic evaluation of low back pain with emphasis on imaging. Ann Intern Med 2002;137:586‑97.
7. Oniankitan O, Magnan A, Fianyo E, Mijiyawa M. Lumbar spinal stenosis in an outpatient clinic in Lome, Togo. Med Trop (Mars) 2007;67:263‑6.
8. Walker BF. The prevalence of low back pain: A systematic review of the literature from 1966 to 1998. J Spinal Disord 2000;13:205‑17.
9. Katz JN. Lumbar disc disorders and low‑back pain: Socioeconomic factors and consequences. J Bone Joint Surg Am 2006;88(Suppl 2):21‑4.
10. Araoye MO. Research Methodology with Statistics for Health and Social Sciences. Vol. 115. Ilorin: Nathadex Publisher; 2003. p. 25‑120.
11. Omokhodion FO. Low back pain in urban population in South West Nigeria. Trop Doct 2004;34:17‑20.
12. Chad DA. Lumbar spinal stenosis. Neurol Clin 2007;25:407‑18.
13. Adeyinka AO, Omidiji OA. Magnetic Resonance Imaging Diagnoses in the lumbar spine of adults with low back pain in South West, Nigeria.
WAJR 2011;18:1‑9.
14. Umerah CK. Magnetic Resonance Imaging Evaluation of low back pain in adult Nigerians at the National Hospital Abuja, Nigeria . FMCR
Dissertation. National Postgraduate Medical College of Nigeria. November 2014.
15. Woolf AD, Pfleger B. Burden of major musculoskeletal conditions. Bull World Health Organ 2003;81:646‑56.
16. Johannessen W, Vresilovic EJ, Wright AC, Elliott DM. Intervertebral disc mechanics are restored following cyclic loading and unloaded recovery. Ann Biom Eng 2004;32:70‑6.
17. Euro U, Knekt P, Rissanen H, Aromaa A, Karppinen J, Heliövaara M. Risk factors for sciatica leading to hospitalization. Eur
Spine J 2018;27:1501‑8.
18. Sanderson SP, Houten J, Errico T, Forshaw D, Bauman J, Cooper PR. The unique characteristics of “upper” lumbar disc herniations.
Neurosurgery 2004;55:385‑9.
19. Christian W. A, Pfirrmann, Claudio Dora. MR Image–based Grading of lumbar nerve root compromise due to disk herniation: Reliability
study with surgical correlation. Radiology 2004;230:583‑8.
20. Jacobson JA, Girish G, Jiang Y, Resnick D. Radiographic evaluation of arthritis: Inflammatory conditions. Radiology 2008;248:378‑89.
21. Walter S, Bartynskia LL. Lumbar root compression in the lateral recess Imaging. MRI, Conventional Myelography, and CT Myelography
comparison with surgical confirmation. Am J Neuroradiol 2003;24:348‑60.
22. Güner G, Elmalı N, Ertem K. Lumbal Spinal Stenoz. J Inonu Univer Med Fac 2010;4:236‑42.
23. Saberi H, Isfahani AV. Higher preoperative Oswestry Disability Index is associated with better surgical outcome in upper lumbar disc
herniations. Eur Spine J 2008;17:117‑21.