

Histopathological characteristics of gynaecomastia in Southwestern Nigeria: A review from a tertiary hospital
Article Sidebar
Abstract Views | PDF/EPUB Downloads: 2012 / 340 / 284
Main Article Content
Abstract
Background: Gynaecomastia is a benign proliferation of the glandular tissue of the male breast. It is thought to be present in at least a third of men in the course of their lifetime. This study aims to review the histomorphological characteristics of gynaecomastia seen at the department of Pathology, University College Hospital (UCH), Ibadan, over 10 years period.
Methods: A hospital-based retrospective study was undertaken to review the histopathology reports of all gynaecomastia cases diagnosed at the Department of Pathology, UCH Ibadan, over a 10-year period from 01 January, 2009 to 31 December, 2018. Patient’s biodata, histological diagnosis and clinical details were extracted from the surgical day books and laboratory request forms. The data were analysed for the frequency distribution using the SPSS software version 22.
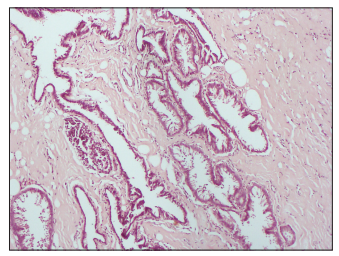
Results: Gynaecomastia accounts for 2.5% of all breast biopsies received within the study period and accounted for 68.1% of all benign breast lesions seen in males. The left breast was the most affected with 48.8% of the cases, whereas 17.2% of the cases were bilateral. The age range of patients with gynaecomastia seen in this study is between 12 and 80 years with a mean age of 43.36 years. The most common histopathological subtype seen in this study is the florid type gynaecomastia.
Conclusion: Gynaecomastia is the most common diagnosis from male breast biopsies. The left breast is the most commonly affected breast. The florid type gynaecomastia is the main histopathological variant seen in this study.
Downloads
Article Details
The journal grants the right to make small numbers of printed copies for their personal non-commercial use under Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported License.
References
1. Carlson HE. Approach to the patient with gynecomastia. J Clin Endocrinol Metab 2011;96:15‑21.
2. Kanakis GA, Nordkap L, BangAK, CalogeroAE, Bártfai G, Corona G, et al. EAA clinical practice guidelines‑gynecomastia evaluation and
management. Andrology 2019;7:778‑93.
3. Rahmani S, Turton P, Shaaban A, Dall B. Overview of gynecomastia in the modern era and the Leeds Gynaecomastia Investigation algorithm.
Breast J 2011;17:246‑55.
4. McKiernan JF, Hull D. Breast development in the newborn. Arch Dis Child 1981;56:55‑9.
5. Nydick M, Bustos J, Dale JH Jr., Rawson RW. Gynecomastia in adolescent boys. JAMA 1961;178:449‑54.
6. Arya R, Rathi AK, Singh K, Srivastava A, Panda D, Parida SN, et al. Gynecomastia: A review of literature. MAMC J Med Sci 2016;2:69‑75.
7. Niewoehner CB, Nuttal FQ. Gynecomastia in a hospitalized male population. Am J Med 1984;77:633‑8.
8. Andersen JA, Gram JB. Male breast at autopsy. Acta Pathol Microbiol Immunol Scand A 1982;90:191‑7.
9. Cuhaci N, Polat SB, Evranos B, Ersoy R, Cakir B. Gynecomastia: Clinical evaluation and management. Indian J Endocrinol Metab 2014;18:150‑8.
10. Williams MJ. Gynecomastia. Its incidence, recognition and host characterization in 447 autopsy cases. Am J Med 1963;34:103‑12.
11. Barros AC, Sampaio Mde C. Gynecomastia: Physiopathology, evaluation and treatment. Sao Paulo Med J 2012;130:187‑97.
12. Bulun SE, Fang Z, Gurates B, Tamura M, Yilmaz B, Amin S, et al. Aromatase in health and disease. Endocrinologist 2003;13:269‑76.
13. Melo KF, Mendonca BB, Billerbeck AE, Costa EM, Inácio M, Silva FA, et al. Clinical, hormonal, behavioral, and genetic characteristics of
androgen insensitivity syndrome in a Brazilian cohort: Five novel mutations in the androgen receptor gene. J Clin Endocrinol Metab 2003;88:3241‑50.
14. Niewoehner CB, Schorer AE. Gynaecomastia and breast cancer in men. BMJ 2008;336:709‑13.
15. Nuttall FQ. Gynecomastia as a physical finding in normal men. J Clin Endocrinol Metab 1979;48:338‑40.
16. Senger JL, Chandran G, Kanthan R. Is routine pathological evaluation of tissue from gynecomastia necessary? A 15‑year retrospective
pathological and literature review. Plast Surg (Oakv) 2014;22:112‑6.
17. Koshy JC, Goldberg JS, Wolfswinkel EM, Ge Y, Heller L. Breast cancer incidence in adolescent males undergoing subcutaneous mastectomy
for gynecomastia: Is pathologic examination justified? A retrospective and literature review. Plast Reconstr Surg 2011;127:1‑7.
18. Lapid O, Jolink F, Meijer SL. Pathological findings in gynecomastia: Analysis of 5113 breasts. Ann Plast Surg 2015;74:163‑6.
19. Hamady ZZ, Carder PJ, Brennan TG. Atypical ductal hyperplasia in male breast tissue with gynaecomastia. Histopathology 2005;47:111‑2.
20. McLaughlin CS, Petrey C, Grant S, Ransdell JS, Reynolds C. Displaced epithelium after liposuction for gynecomastia. Int J Surg Pathol 2011;19:510‑3.
21. Braunstein GD. Clinical practice. Gynecomastia. N Engl J Med 2007;357:1229‑37.
22. Irabor DO, Okolo CA. Outcome of one hundred and forty‑nine consecutive breast biopsies in Ibadan, Nigeria. Breast Dis 2011;33:109‑14.
23. Ibrahim IM, Iliyasu Y, Mohammed AZ. Histopathological review of breast tumors in Kano, Northern Nigeria. Sub‑Saharan Afr J Med
2015;2:47‑51.
24. Yusufu LMD, Odigie VI, Mohammed A. Breast masses in Zaria, Nigeria. Ann Afr Med 2003;2:13‑6.
25. Olsson H, Bladstrom A, Alm P. Male gynecomastia and risk for malignant tumours—a cohort study. BMC Cancer 2002;2:26.
26. Liao EC, Kish JB, Hertl MC. Incidental discovery of bilateral breast cancer in a 24‑year‑old man presenting with gynecomastia. Ann Plast
Surg 2007;58:673‑6.
27. Ersöz Hö, Onde ME, Terekeci H, Kurtoglu S, Tor H. Causes of gynaecomastia in young adult males and factors associated with idiopathic gynaecomastia. Int J Androl 2002;25:312‑6.